Why add an essential oil antiseptic mouthrinse to your patients’ daily oral health routine?
Even with today’s increased focus on oral healthcare, including good brushing and flossing techniques, gum disease is still much more prevalent than might be expected. In fact, in Canada alone, 88% of adults aged 20 years and older exhibit signs of gum inflammation and 32% actually have gingivitis.1 It’s important to understand what comprises your patient’s typical daily oral care routine so that you can counsel them on ways to improve their oral health outcomes.

The good news is the majority of people are willing to do more for their oral health. A global survey of over 4,000 people5* showed:

It’s clear that patients already have the desire to improve their oral health, but need a better understanding of the state of their current oral health, their relative risk of gingivitis, and require education on an individualized home regime.
Why recommend oral rinsing?
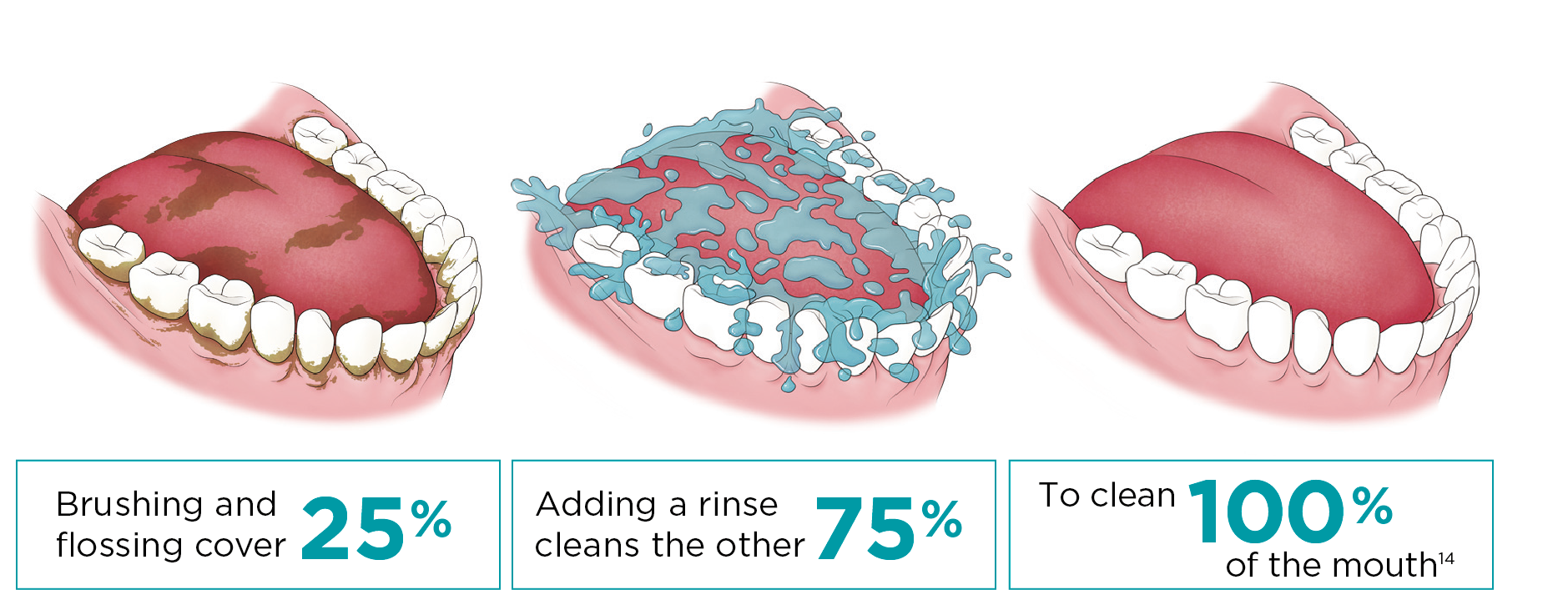
While mechanical methods, like brushing and flossing, are vital to proper oral care, they may not be enough on their own to control plaque.6,7 Bacteria are hiding in places where brushing, and even flossing, simply can’t reach. Appearing within minutes of brushing, bacteria double every 1–2 hours in the early stages—and within days, microbes form a complex 3-D colony that can contain hundreds of distinct species.8† Unstimulated saliva contains 5 x 107 to 1 x 108 bacteria per millilitre, and continually bathes oral surfaces with suspended microorganisms, allowing bacteria to re-colonize on teeth shortly after prophylaxis.9 In just 30 seconds, the antimicrobial action of an essential oil mouthrinse reduces plaque left behind by mechanical methods, deeply penetrating into the bottom layers of the biofilm, breaking down its structure in places that are more difficult for a toothbrush and dental floss to access.10,11,12

CDA and CDHA recognizes the benefits of rinsing.15, 16
In addition to the Canadian Dental Association recommendation for brushing and flossing, the have evaluated the clinical benefits provided by rinsing with an antiseptic essential oil containing mouthrinse. The CDA has validated the oral health benefit that adding LISTERINE® Antiseptic to one’s oral routine reduces and prevents gingivitis more than just brushing and flossing alone.
Rinsing—the essential third step to better oral health.
With all this evidence, it’s clear that rinsing with an antiseptic mouthrinse is more than just a suggestion, it is an essential third step in addition to brushing and flossing in a patient’s daily oral health routine. And it’s a step you should be recommending to your patients to help make their mouths healthier.
Test your knowledge?
1. What is the prevalence of gingivitis in Canada?
a.) Over 10% of the adult population
b.) Over 30% of the adult population
c.) Over 50% of the adult population
d.) Over 85% of the adult population
2. What is the benefit of using antiseptic mouthrinse in addition to mechanical methods of plaque removal?
a.) Helps prevent and reduce plaque
b.) Helps prevent and reduce gingivitis
c.) Clean virtually 100% of the mouth
d.) All of the above
3. What percentage of clients are willing to use mouthwash for improved oral health?
a.) 90 %
b.) 50 %
c.) 25 %
d.) 10 %
Answers: 1. b; 2. d; 3. a

CLINICAL STUDIES ON PLAQUE AND GINGIVITIS REDUCTION
Explore evidence from a study about LISTERINE® Antiseptic and the reduction of plaque and gingivitis.
THE CDA RECOGNIZE THE BENEFITS OF RINSING*
CDA validates that adding LISTERINE® antiseptic mouthwash to a regular oral hygiene routine reduces and prevents gingivitis more than brushing and flossing alone.
*Based on self-reported data from a survey of patients in the United States, United Kingdom, Thailand, Brazil and Japan (N=4134).
†25 species at a specific location in the biofilm, but several hundred species throughout the mouth of the same individual.
1. Health Canada, Canadian Health Measures Survey 2007-2009. 2.. Bakdash B. Current patterns of oral hygiene product use and practice. Periodontal 2000. 1995;8:11-14. 3. Cancro LP, Fischman SL. The expected effect on oral hygiene of dental plaque control through mechanical removal. Periodontology 2000. 1995;8:60-74. 4. Bader HI. Floss or die: implications for dental professionals. Dent Today. 1998;17:76-82. 5. Based on self-reported data from a survey of people in the United States, United Kingdom, Thailand, Brazil and Japan (N=4134), data on file Johnson & Johnson Inc. 2015 6. Gunsolley JC. A meta-analysis of six-month studies of antiplaque and antigingivitis agents. JADA. 2006;137:1649-1657. 7. Gunsolley JC. Clinical efficacy of antimicrobial mouthrinses. J Dent. 2010;38(I):S6-S10. 8. Marsh PD. Martin MV, Lewis MOA, Williams D. Dental Plaque. Oral Microbiology E-Book, 5th Edition. Churchill Livingstone. 2009. 80-89. 9. Liljemark WF, Bloomquist CG, Reilly BE, Lemoine JL. Growth dynamics in a natural biofilm and its impact on oral disease management. Adv Dent Res. 1997;11(1):14-23. 10. Foster JS, Pan PC, Kolenbrander PE. Effects of antimicrobial agents on oral biofilms in a saliva-conditioned flowcell. Biofilms. 2001;1:512. 11. Minah GE, DePaola LG, Overholser CD, et al. Effects of 6 months use of an antiseptic mouthrinse on supragingival dental plaque microflora. J Clin Periodontol. 1989;16:347-352. 12. Walker C, Clark W, Wheeler T, Lamm R. Evaluation of microbial shifts in supragingival plaque following long-term use of an oral antiseptic mouthrinse. J Dent Res. 1989;68:412. 13. Data on File. Johnson & Johnson Consumer Inc. 14. Kerr WJS, Kelly J, Geddes DAM. The areas of various surfaces in the human mouth from nine years to adulthood. J Dent Res. 1991; 70:1528-1530. 15. https://www.cda-adc.ca/en/oral_health/seal/about/ 16. http://www.cdha.ca/pdfs/Profession/Resources/TherapeuticOralRinsingPartI.pdf
Please Note: Some of the links in this article may take you to websites to which our privacy policy does not apply. You are solely responsible for your interactions with those websites. We encourage you to read the privacy policy of every website you visit.
This communication is intended for visitors from Canada only and is subject to the terms of our Legal Notice and Privacy Policy